Anterior Cervical Fusion Surgery
Anterior Cervical Spine Surgery
Cervical Spondylosis is a very common degenerative spine disorder. Mostly elderly people are affected; however, it can affect younger patients also. Anterior Cervical Fusion is gold standard procedure for these patients. Cervical spine is approached from the front. Anterior cervical fusion can be divided in 1) Anterior Cervical Discectomy and Fusion (ACDF), and 2) Anterior Cervical Corpectomy and Fusion (ACCF).
Anterior Cervical Discectomy and Fusion (ACDF):
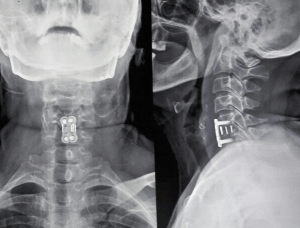
ACDF involves removal of cervical disc/ discs and reconstructing the space with a bone graft/ cage/ anterior cervical plate or a combination of these. This is procedure of choice when disc and osteophytes are bulging in spinal canal and causing pressure on spinal cord. A multilevel ACDF can be done depending upon the number of discs affected.
Anterior Cervical Corpectomy and Fusion (ACCF):
ACCF involves removal of cervical vertebra/ vertebrae, either partially or completely. An ACCF is required when spinal cord is compressed behind the vertebral body, which cannot be approached by cervical discectomy. Some surgeon’s prefer doing an ACCF rather than multilevel ACDF to tackle multilevel cervical spinal cord compression.



Indications of Anterior Cervical Fusion Surgery:
- Cervical Spondylosis: Causing severe neck pain, not responding to medical treatment.
- Cervical Radiculopathy: Compression of cervical spinal nerve causing pain, tingling-numbness, sensory changes, muscle weakness in upper limbs.
- Cervical Myelopathy: Patients who have feature of myelopathy (hand grip weakness, clumsiness of hand functions, loss of body balance, difficulty in walking, stiffness in arms and legs, loss of bladder-bowel control).
- Cervical Spine Fractures.
- Cervical Spine Infection/ Tuberculosis.
- Cervical Spine Tumors.
Advantages of Anterior Cervical Spine Fusion Surgery:
- A minimally invasive procedure.
- Very well tolerated by patients.
- Targets the pathology (disc, osteophytes etc.) directly.
- Very safe and effective procedure.
- Very unlikely to cause any major side effects.
Side effects of Anterior Cervical Spine Fusion Surgery:
ACDF and ACCF are both very safe surgeries. However, like any other surgery, common complications, e.g. pain, infection, hematoma etc. can happen. Even these are extremely rare with anterior cervical fusion surgeries as significant soft tissue and muscle dissection are not required when cervical spine is approached from the front. Some difficulty in swallowing can be experienced by the patients due to close proximity to oesophagus (food pine passing through the neck to stomach). This happens in the immediate post-operative period and usually resolves within 3-4 days. Hoarseness of voice is another rare complication which can occur due to irritation of nerve supplying vocal cords (voice box situated in neck). Again, this is usually a self-resolving condition.
Recent Advances:
- Stand Alone Cage: Conventionally, ACDF is done using a cage in interbody area from where disc is removed, which is supported by a plate applied on anterior surface of cervical spine. Plate can irritate oesophagus and other soft tissues in neck causing pain of swallowing in some cases. This is avoided by using a stand-alone cage as it is fixed by screws passing through the cage itself.
- Minimally Invasive Anterior Cervical Spine Fusion Surgeries: ACDF and ACCF can be done following minimally invasive spine surgery principles using specialized retractors and microscope.
- Disc Replacement Surgery: Cervical disc replacement is an alternative to ACDF, especially in young age patients. This will maintain motion at operated level and will reduce chances of adjacent segment degeneration(ASD).
Spinal interbody discs are not been given any particular name. They are known by the name/ number of the vertebral bones surrounding them. C5-6 is the name of the disc between C5 and C6 vertebra. In the cervical spine, there is C2-3, C3-4, C4-5, C5-6 and C6-7 discs present.
Spinal discs are soft cartilage structure. They are subjected to wear and tear by aging process and motion. C5-6 disc gets maximum movement during day to day activities due to its center location. Hence, majority of the patients suffering from cervical spondylosis and cervical disc prolapse will have C5-6 pathology. However, it is very common for the patients to have C6-7 and C4-5 spondylosis also requiring spine surgery.
Recovery after anterior cervical fusion surgery is very fast and smooth. Patients are able to sit and walk on the day of surgery. Majority of the patients with 1-2 level ACDF can be discharged day after surgery.Patients with 3-4 level ACDF or ACCF might have to stay in the hospital for 2-3 days.
Arm pain is resolved immediately after the surgery. However, numbness and weakness might take long time to resolve after anterior cervical fusion surgery.
Some amount of surgical pain is present for few days. However, it is in the bearable range.
Dysphagia is difficulty in swallowing. Almost all patients feel some amount of dysphagia after anterior cervical spine surgery. This is similar to muscle soreness after back surgery. This dysphagia is usually mild and resolves within 2-3 days. Patients are able to swallow semi-solid foods better than the liquids.
Rarely, dysphagia can last longer. In this situation, a careful assessment of patient’s throat is required by an ENT specialist and any major injury to nerves supplying the swallowing muscles need to be ruled out. A vocal cord examination is also required to prevent a risk of aspiration.
Success rate of anterior cervical fusion procedure is very high. It is a spine surgeon’s favorite surgery due to predictable outcome with almost immediate relief in patients’ symptoms. These surgeries are easy on the patients as majority of these surgeries are minimally invasive and does not require major soft tissue dissection.
Cost of ACDF depends on following factors
- Number of discs levels involved
- Pathology of disc prolapse (acute soft disc prolapse vs hard osteophyte/ OPLL)
- Type of spinal implant used (Indian/ Imported)
- Type of hospital (small vs big hospital)
- Type of room patients chooses (multisharing/ twin sharing/ single occupancy private room)
In general, cost is approximately 2,00,000 Indian Rupees for a multi-sharing general ward room for a single level disc prolapse with an Indian prosthesis. This cost can go up to 6,00,000-7,00,000 Indian Rupees for a single occupancy room with imported prosthesis for a single level cervical disc prolapse.