Spondylolisthesis
Spondylolisthesis: Diagnosis and Treatment
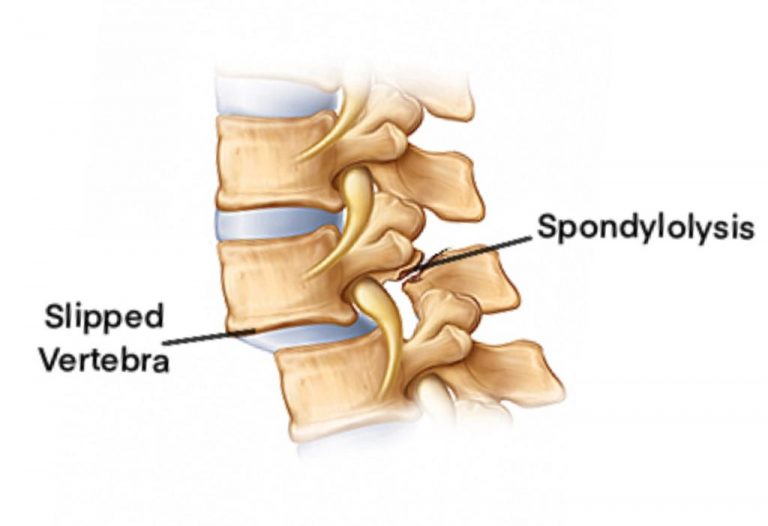
Spondylolisthesis (spondylo= spine, listhesis= slip or slide) is a common spinal problem in which one vertebra slips forward on the vertebra below. Primary reason behind spondylolisthesis is spondylosis, which causes loss of functions of joints (disc and facets) holding two vertebrae together. Spondylolisthesis may be associated with spinal instability, wherein there is excessive abnormal movements between two vertebrae.
Spondylolysis:
Sometimes there is a fracture of the posterior part of the vertebra (Spondylolysis or pars-interarticularis fracture, commonly known as pars defect). This causes break in hook mechanism which holds upper vertebra in place over lower vertebra.
Spondylolisthesis primarily affects lumbar spine; however, cervical spine can also be affected. It is divided in various grades depending upon percentage of slip of upper vertebra. A higher grade listhesis is more likely to cause more symptoms.

Spondylolysis Symptom:
Symptoms of spondylolisthesis depends on its grade and duration. Primary symptom is pain at the local site due to associated spondylosis. Majority of cases have associated spinal stenosis also, which occurs due to 1) usual degenerative changes in spine, and 2) loss of continuity of spinal canal due to mal-aligned vertebrae. Spinal stenosis can cause spinal cord/ nerves pressure related symptoms (radiculopathy in arms/ legs, tingling-numbness, loss of sensation, weakness in muscles, loss of hand grip, loss of body control, tightness in body, loss of bladder-bowel control) .
Spondylolysis Diagnosis:
Spondylolisthesis is diagnosed by following tests:
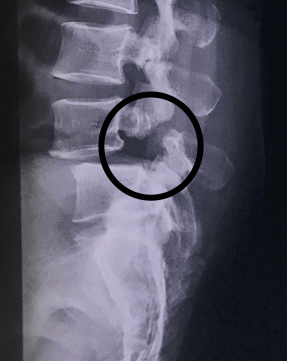
- X-ray: An x-ray will show slip of vertebra. Grading of spondylolisthesis is done on x-rays. X-ray will also show signs of spondylosis (loss of disc height, vertebral bony spur formation). In patients with spondylolysis, fracture in pars interarticularis can also be seen on x-ray. An x-ray in different positions (flexion-extension) can also reveal associated spinal instability, which might be missed on static imaging, like MRI.
- MRI Scan: It will show listhesis of vertebra along with usual degenerative changes of spondylosis. Severity of spinal stenosis will also be assessed on MRI scan.
- CT Scan: A CT scan is sometimes required to confirm/ rule out pars interarticularis fracture. CT scan will also give additional information about bony anatomy in detail.
- Other tests, like EMG-NCV, blood tests etc, might be required to confirm or rule out any associated pathology.
Spondylolysis Treatment:
- Medical Treatment: Like any other spine condition, initial treatment of spondylolisthesis is primarily by medicines, local heat/ ice, bracing, activity restriction and physiotherapy. Patients with mild symptoms and lower grade slip usually responds well to medical treatment. Physiotherapy helps build muscle strength and relieves muscle spasm. Stronger muscle will act as an internal brace and will also prevent excessive motion at painful spinal segment.
- Pain Management/ Epidural Injection: Various pain management procedures targeting disc (intra-discal steroid injection, LASER disc therapy), facet joint (facet injection, Radio-Frequency nerve ablation) or the spinal cord (epidural injection) can be done. These procedures are done to provide pain relief. They do not reverse listhesis or degenerative changes in spine.
- Spondylolisthesis Surgery: Patients who do not respond to medical treatment/ pain management and have severe symptoms usually need spine surgery. A patient with mild grade of listhesis with no significant back pain and primarily having spinal cord pressure symptoms might need only spine decompression surgery. However, simultaneous spine fusion/ instrumentation surgery is recommended in following situations:
- Spondylolysis (pars interarticularis fracture),
- Significant spinal instability (as judged on flexion/ extension x-rays),
- Significant pain in spine due to spondylosis,
- High grade listhesis (to prevent further progression),
- In cases where excessive/ crucial part of the bone/ joint need to be removed to achieve adequate spinal cord decompression,
- Associated spinal deformity.
There are situations when a spine fusion/ instrumentation surgery is contra-indicated/ better avoided (even if required):
- Severe osteoporosis: spinal implant will not hold firmly in weak bone and bone fusion will also take long time,
- Associated severe medical problems: As spine instrumentation make surgery bigger, it is better avoided in patients with multiple medical problems,
- Patients with main symptoms of spinal cord pressure and not having any of the above mentioned indication for a spine fusion surgery, as a spine fusion/ instrumentation will unnecessarily make surgery bigger with added risk of instrumentation, extra expenses and longer recovery time.
Majority of the surgical procedures can be done now with minimally invasive/ key hole techniques with the advantage of minimal blood loss during surgery, minimal pain medicines requirement after the surgery, faster recovery and rehabilitation, short hospital stay and a cosmetic scar.
Frequently asked questions:
Spondylolisthesis involves vertebral slippage, spondylosis refers to degenerative spine changes, and spondylolysis is a defect in the pars interarticularis. Exploring these differences can help in better understanding these spinal conditions.
Spondylolysis symptoms typically include lower back pain, while spondylolisthesis may also cause radiating pain, muscle weakness, and changes in gait. These conditions can have varying degrees of impact on daily activities.
Spondylolisthesis exercises focus on strengthening core and back muscles, improving flexibility, and reducing pain. A tailored exercise program, recommended by a healthcare professional, can help alleviate discomfort.
Surgery may be considered for severe cases or when conservative treatments fail. Procedures may involve spinal fusion, decompression, or pars repair, depending on the specific condition and its severity.
Bilateral spondylolysis at L5-S1 involves defects on both sides of the vertebra, potentially leading to spondylolisthesis. This condition can manifest as lower back pain and discomfort during activities that stress the lumbar spine.
Spondylolisthesis is graded based on the extent of vertebral slippage, ranging from mild (Grade 1) to severe (Grade 5). These grades help determine the severity of the condition and guide treatment decisions.
The pars interarticularis is a bony bridge crucial to spinal stability. Spondylolysis occurs when there’s a defect in this structure, which can lead to spondylolisthesis if left untreated.
Spondylolysis is often caused by repetitive stress on the pars interarticularis and may be associated with activities involving hyperextension of the spine, such as certain sports. It occurs more frequently at the L5 level due to its high mobility and the stress it experiences.
High-resolution imaging like MRI and CT scans provide detailed views of the spine, crucial for accurate diagnosis and planning of surgical interventions.
Spondylolysis surgery is typically considered in cases of severe pain or if conservative treatments are ineffective. Surgical options may include a pars repair procedure or spinal fusion to address the pars defect.